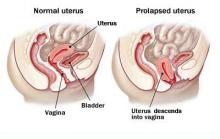
PROLAPSE - WHAT IS IT?
Prolapse occurs when the muscles, ligaments and fascia (a network of supporting tissues) holding the internal organs in place become weakened. This allows one or more organs to drop out or “Prolapse” into the vagina. Think of the pelvic floor like a trampoline – prolapse may happen if there is a split or tear in the mat, springs (ligaments) become overstretched or tear away. It affects about 1 in 3 women.
DO I HAVE IT? HOW WILL I KNOW?
Many women have minor prolapse and feel completely fine. Common complaints are a lump, dragging discomfort especially after a long day, problems with emptying bladder or bowels. Leaking of urine with coughing or jumping can occur.
WHAT CAUSES PROLAPSE?
Pregnancy and childbirth are the major factors. It can occur soon after birth or years later. Age and menopause further weaken tissues. Inherited weakness of connective tissues can contribute as can chronic cough or constipation, heavy lifting, obesity and smoking.
WHAT SHOULD I DO IF WORRIED?
See your doctor for review. Some may worry that a new lump is cancer. Often only an explanation is needed. Options for treatment can be discussed including physiotherapy, pelvic floor exercises or a pessary. Surgery may be considered for more severe cases.
WHAT KIND OF SURGERY?
This will depend on what is dropping down and how severe it is. Are you troubled by it? A person with no symptoms will not benefit from an operation. You need to discuss your case with your doctor. Surgery will try to repair your tissues and restore normal function. Depending on severity and other factors including whether this is the first operation or a recurrent problem mesh may be considered. This can be synthetic or derived from animal tissue.
WHAT IS THE MESH MADE FROM?
The synthetic mesh is made from polypropylene which is used in many surgical implants including mesh for hernia repairs and aortic grafts. The type of mesh weave and density varies with the place it is placed. Vaginal mesh is generally lighter and more flexible. Biologic mesh is derived from animal tissue and will dissolve over some months.
WHY IS IT USED?
Prolapse occurs in many women and recurrence after surgery is also common, at least 40% and up to 90% in some groups. The desire to decrease prolapse recurrence by helping reinforce weak tissues was the driving force behind the development of mesh.
ARE SLINGS THE SAME?
Current bladder (Mid-urethral) slings are synthetic. There are several types which vary in where they are inserted and fixed. Slings have been used for many years and in the past were made from various synthetics, sutures or your own tissue (fascia cut from the side of the leg or abdominal wall).
THE HISTORY OF MESHES
The use of mesh is not new. In 1955 an artificial mesh was first used for bladder prolapse. It became more popular however after the success of bladder (mid-urethral slings) in the 1990’s. Several new products became available from 2003-2004 onwards leading to increased use.
I hear talk of mesh in the media lately.
I HEAR TALK OF MESH IN THE MEDIA LATELY. WHAT ARE THE PROBLEMS?
All surgery has a risk of complications including bleeding, infection, damage to nearby structures and an anaesthetic. Chronic pain and pain with intercourse is reported. Those with pain prior to surgery should fix this first as it may get worse. Risks will vary for each individual and are best discussed with your doctor. The only specific risk associated with mesh use is erosion where small areas may become exposed in the vagina. This has been reported in 5-10 % of cases. Sometimes it gives no problems and can be left. Sometimes small area are excised and closed over. The risk is higher if post-menopausal with thin tissue so local estrogen is often recommended.
WHAT SHOULD I DO IF I HAVE A MESH?
Hopefully you are continuing regular check-ups with your doctor. This will mean if problems develop they can advise you. If you are well there is no need to do anything different. Specific problems should be discussed with them.
Hundreds of thousands of meshes and slings have been used worldwide and have given many women relief from their prolapse and incontinence.
An open honest discussion with your doctor is the best way forward prior to considering any treatment.
WANT TO KNOW MORE?
Click on the following link to the Royal Australian and New Zealand College of Gynaecologists website to hear Dr Steve Robson explain more about gynaecological mesh.
http://bit.ly/2wsKrtu